Have you ever wondered what your hormones are actually doing throughout your cycle?
Many women hear terms like estrogen, progesterone, LH, FSH, ovulation tests, or hormone panels, yet few receive a clear explanation of how these pieces fit together.
In reality, the menstrual cycle is a remarkable biological conversation between the brain, the ovaries, and the uterus. Every hormonal rise and fall serves a purpose. Every phase of the cycle tells a story.
Understanding these hormonal patterns can help you make better sense of:
-
Cervical mucus changes
-
Ovulation tests
-
Basal body temperature charts
-
Blood test results
-
Fertility awareness tracking
-
Pregnancy tests
-
Irregular cycles
-
Conditions such as PCOS
Let’s explore what is happening behind the scenes
The Hormonal Control Center
The menstrual cycle is controlled by what scientists call the Hypothalamic-Pituitary-Ovarian (HPO) Axis.
Think of it as a communication network.
The Hypothalamus
Located in the brain, the hypothalamus acts as the master coordinator.
It releases Gonadotropin-Releasing Hormone (GnRH) in small pulses.
These pulses tell the pituitary gland how much FSH and LH to produce.
The Pituitary Gland
The pituitary gland sits just beneath the brain.
It produces:
-
FSH (Follicle Stimulating Hormone)
-
LH (Luteinizing Hormone)
These hormones travel through the bloodstream to the ovaries.
The Ovaries
The ovaries respond by producing:
-
Estrogen
-
Progesterone
These hormones influence:
-
The uterus
-
Cervical mucus
-
Breasts
-
Bones
-
Metabolism
-
Mood
-
Energy levels
-
Libido
-
Fertility
The ovaries then send hormonal feedback back to the brain.
The entire cycle depends on this ongoing conversation.
FSH: The Follicle Recruiter
FSH stands for Follicle Stimulating Hormone.
Its primary job is to recruit follicles in the ovaries.
Each follicle contains an immature egg.
At the beginning of the cycle, FSH rises slightly and stimulates a group of follicles to begin growing.
Usually only one follicle becomes dominant.
This dominant follicle will eventually release the egg during ovulation.
As the dominant follicle grows, it becomes more sensitive to FSH and produces increasing amounts of estrogen.
Once estrogen reaches sufficient levels, the brain gradually reduces FSH production, and the other follicles degenerate.
This prevents too many follicles from continuing development at the same time.
AMH: A Window Into Ovarian Reserve
You may have heard of a hormone called AMH (Anti-Müllerian Hormone), which is often measured during fertility evaluations.
Unlike FSH, AMH does not directly control the menstrual cycle.
Instead, it provides information about the number of small growing follicles present in the ovaries.
Many people believe that AMH (Anti-Müllerian Hormone) measures the total number of eggs remaining in the ovaries. However, the reality is a little more complex.
AMH is not produced by dormant eggs resting in the ovarian reserve. Instead, it is produced by the granulosa cells of small, newly developing follicles. These follicles have left the resting pool and entered the early stages of growth, long before one of them becomes the dominant follicle of the cycle.
Because small developing follicles continuously emerge from the ovarian reserve, AMH provides an indirect estimate of it. In general, women with a larger remaining pool of eggs tend to have more small growing follicles and therefore higher AMH levels. As the ovarian reserve declines with age, fewer follicles enter the growth phase, and AMH levels typically decrease.
It is important to understand that AMH does not provide an exact count of remaining eggs, nor does it measure egg quality. Instead, it serves as a useful marker of the ovary’s remaining reproductive potential by reflecting the number of small follicles currently available for future development.
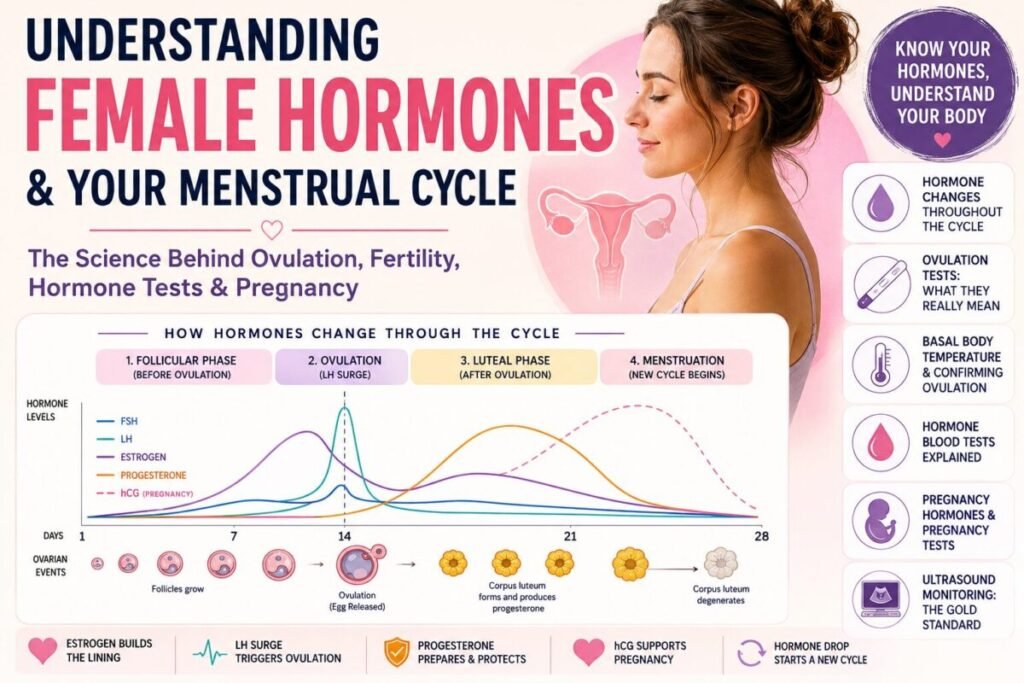
Estrogen: The Builder
Estrogen is primarily produced by the developing follicle.
As ovulation approaches, estrogen levels rise steadily.
Estrogen’s job is to prepare the body for potential conception.
It helps:
-
Build the uterine lining
-
Improve blood flow
-
Increase cervical mucus production
-
Support bone health
-
Influence mood and cognition
-
Increase energy and motivation
Many women notice that during the follicular phase they feel:
-
More energetic
-
More confident
-
More sociable
-
More motivated
-
More mentally focused
This often reflects the rising influence of estrogen.
How Estrogen Triggers Ovulation
One of the most surprising features of the cycle is that estrogen changes its behavior.
For most of the follicular phase, estrogen tells the brain:
“We have enough follicles. Reduce FSH.”
This is called negative feedback.
However, once estrogen reaches a critical level and remains high for approximately 36 hours, the message changes.
The brain now interprets it as:
“The egg is ready.”
This triggers a dramatic release of LH.
This event is known as the LH Surge.
LH: The Ovulation Trigger
LH stands for Luteinizing Hormone.
Although LH is present throughout the cycle, it suddenly rises 10 to 20 times above baseline levels just before ovulation.
This LH surge initiates several important events:
-
Final maturation of the egg
-
Weakening of the follicle wall
-
Release of enzymes that help rupture the follicle
-
Preparation of the follicle to become the corpus luteum
Approximately 24–36 hours after the LH surge begins, ovulation usually occurs.
The mature egg is released from the ovary and enters the fallopian tube.
The egg remains capable of fertilization for approximately 12–24 hours.
 Did you know about Oogenesis that…
Did you know about Oogenesis that…
 Did you know about Oogenesis that…
Did you know about Oogenesis that…… a woman is born with all her eggs already formed?
- Female eggs begin their development during fetal life, while the baby is still in the womb.
- At this stage, the ovaries already contain around 6–7 million primary oocytes (immature egg cells).
… the number of eggs decreases dramatically before birth?
- By the time a baby girl is born, only about 1–2 million oocytes remain.
- By puberty, this number drops further to around 300,000–500,000.
Most eggs are naturally lost through a process called atresia, in which they stop developing and are reabsorbed by the body.
… only a small fraction of eggs will ever ovulate?
- During reproductive life, only about 300–500 eggs will actually be ovulated.
- The rest never fully mature.
Even though many follicles develop in each cycle (around 10–30), usually only one becomes dominant — the others degenerate due to insufficient hormonal support (primarily FSH and LH sensitivity).
… the dominant follicle that eventually releases the egg is not the main source of AMH.
In fact, AMH production decreases as follicles grow larger and become more mature. Most AMH is produced by the many small follicles that are still in the early stages of development.
… the egg cell division is very unusual?
The egg undergoes a special type of cell division called meiosis (reduction division).
- The first stage of meiosis begins during fetal life but pauses for many years.
- This first division completes only when the egg is ovulated.
… the second meiotic division only happens if fertilization occurs?
- The second part of meiosis is not completed at ovulation.
- It only finishes after the egg is fertilized by a sperm.
This ensures that the egg only becomes a fully mature cell when it is actually needed.
… the egg division is asymmetrical?
Unlike most cells, the egg divides in an uneven way:
- One cell keeps almost all the cytoplasm (nutrients and resources)
- The other becomes a very small structure called a polar body
This is intentional — it ensures that the final egg has enough energy and resources to support early embryo development.
Why Cervical Mucus Changes
The same estrogen that prepares the follicle also affects the cervix.
As ovulation approaches, cervical mucus typically becomes:
-
Clear
-
Stretchy
-
Slippery
-
Similar to raw egg white
This fertile-quality mucus helps sperm survive and travel toward the egg.
Under ideal conditions, sperm can survive in fertile cervical mucus for up to five days.
This is why pregnancy can occur even if intercourse takes place several days before ovulation.
How Ovulation Tests Work
Ovulation predictor kits (OPKs) detect LH in urine.
When LH rises above a certain threshold, the test becomes positive.
A positive test means:
“Your body is preparing to ovulate.”
However, it does NOT prove that ovulation actually occurred.
This distinction is extremely important.
The body can sometimes produce an LH surge without successfully releasing an egg.
This is particularly common in some women with PCOS.
For this reason:
A positive ovulation test predicts ovulation.
It does not confirm ovulation.
Progesterone: The Hormone That Confirms Ovulation
After ovulation, the ruptured follicle transforms into a temporary endocrine gland called the corpus luteum.
The corpus luteum begins producing progesterone.
Many people know progesterone as the “pregnancy hormone.”
But its first and most important role is actually to signal:
“Ovulation has happened.”
Progesterone tells the body to stop preparing new follicles and instead focus on supporting a potential pregnancy.
This is why progesterone acts as a natural “cycle closer.”
Its effects include:
-
Stabilizing the uterine lining
-
Increasing basal body temperature
-
Thickening cervical mucus
-
Promoting relaxation
-
Supporting implantation
A sustained rise in progesterone is one of the strongest biological signs that ovulation truly occurred.
Why Basal Body Temperature Rises
Progesterone has a warming effect on the brain’s temperature regulation center.
As a result, basal body temperature usually rises by approximately 0.2–0.5°C after ovulation.
This temperature shift occurs after the egg has already been released.
Therefore:
Basal body temperature cannot predict ovulation.
However, it can help confirm that ovulation likely occurred.
What Happens If Pregnancy Does Not Occur?
The corpus luteum only survives for about 12–16 days unless it receives a special hormonal signal.
If fertilization and implantation do not occur:
-
The corpus luteum degenerates
-
Progesterone falls
-
Estrogen falls
-
The uterine lining sheds
-
Menstruation begins
The drop in progesterone also removes the signal suppressing FSH.
This allows the brain to begin recruiting follicles for a new cycle.
What Happens If Pregnancy Occurs?
If an embryo successfully implants into the uterine lining, it begins producing a hormone called Human Chorionic Gonadotropin (hCG).
This hormone sends an important message to the corpus luteum:
“Do not shut down. Pregnancy has begun.”
As a result:
- Progesterone remains elevated
- The uterine lining is maintained
- Menstruation does not occur
The corpus luteum continues to produce progesterone and support the pregnancy during the first weeks after conception.
As the placenta develops, it gradually begins producing its own hormones. Between approximately 7–9 weeks of pregnancy, the placenta starts contributing significant amounts of progesterone, and by around 10–12 weeks, it usually takes over as the primary source of hormone production. This transition is known as the luteal-placental shift.
How Pregnancy Tests Work
Most home pregnancy tests can detect pregnancy around the time of a missed period, typically 12–14 days after ovulation.
Pregnancy tests do not measure progesterone.
They do not measure estrogen.
They do not measure LH.
Pregnancy tests detect hCG, the embryo’s first hormonal message to the mother’s body.
After implantation, hCG levels rise rapidly, helping maintain the corpus luteum and its progesterone production until the placenta is ready to take over.
When hCG rises above a detectable level, the pregnancy test becomes positive.
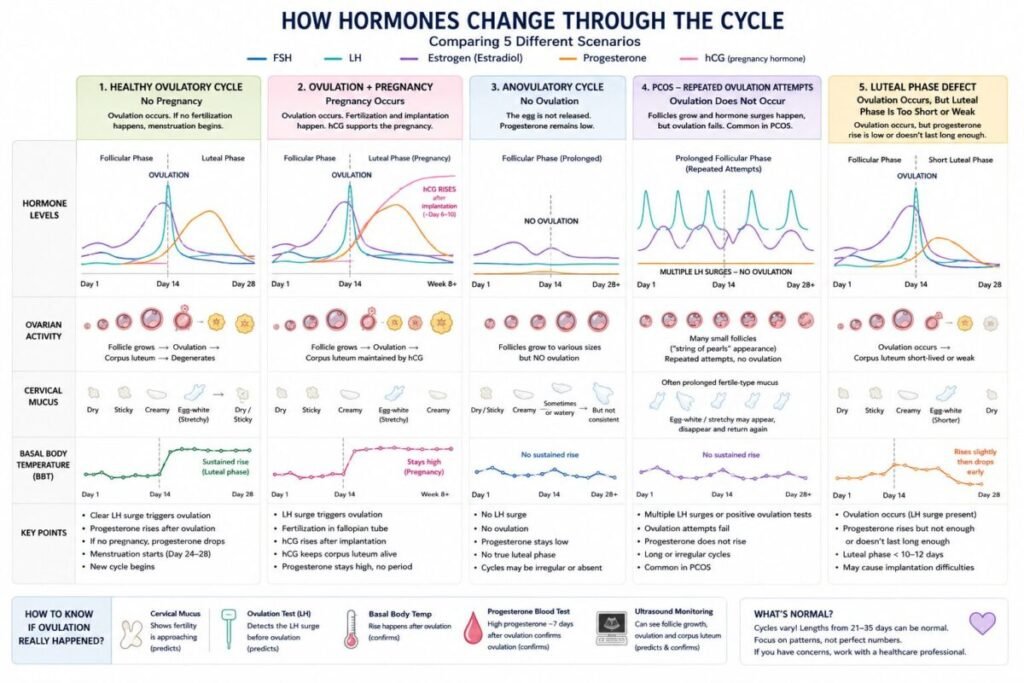
What Happens During an Anovulatory Cycle?
An anovulatory cycle is a cycle in which no egg is released.
Interestingly, some signs of fertility may still appear.
A woman may experience:
-
Cervical mucus
-
Estrogen rises
-
Breast changes
-
Ovulation-like symptoms
However, because no ovulation occurs:
-
No corpus luteum forms
-
Progesterone remains low
-
No true luteal phase develops
The key difference is the absence of a sustained rise in progesterone.
Why PCOS Can Be Confusing
Many women assume:
Positive LH test = ovulation.
However, PCOS often tells a more complicated story.
In some women with PCOS:
-
Follicles begin developing
-
Estrogen rises
-
Fertile cervical mucus appears
-
LH rises
Yet ovulation fails to occur.
The body may then attempt ovulation again days or weeks later.
This can lead to:
-
Multiple LH surges
-
Repeated positive ovulation tests
-
Long cycles
-
Prolonged fertile mucus
-
Multiple patches of egg-white cervical mucus
Many fertility awareness instructors report that women practicing cycle tracking often notice these patterns before receiving a diagnosis.