A Guide to Better Understanding Common Fertility Blood Tests
Unlike many blood tests, reproductive hormones change continuously throughout the menstrual cycle.
A value that is perfectly normal on one day may be completely different a week later.
For this reason, fertility specialists often request blood tests:
Early follicular phase (Day 2–5)
to assess ovarian reserve and hormonal balance.
and
Mid-luteal phase (approximately 7 days after ovulation)
to confirm ovulation and evaluate progesterone production.
Understanding when the blood sample was taken is often just as important as understanding the result itself.
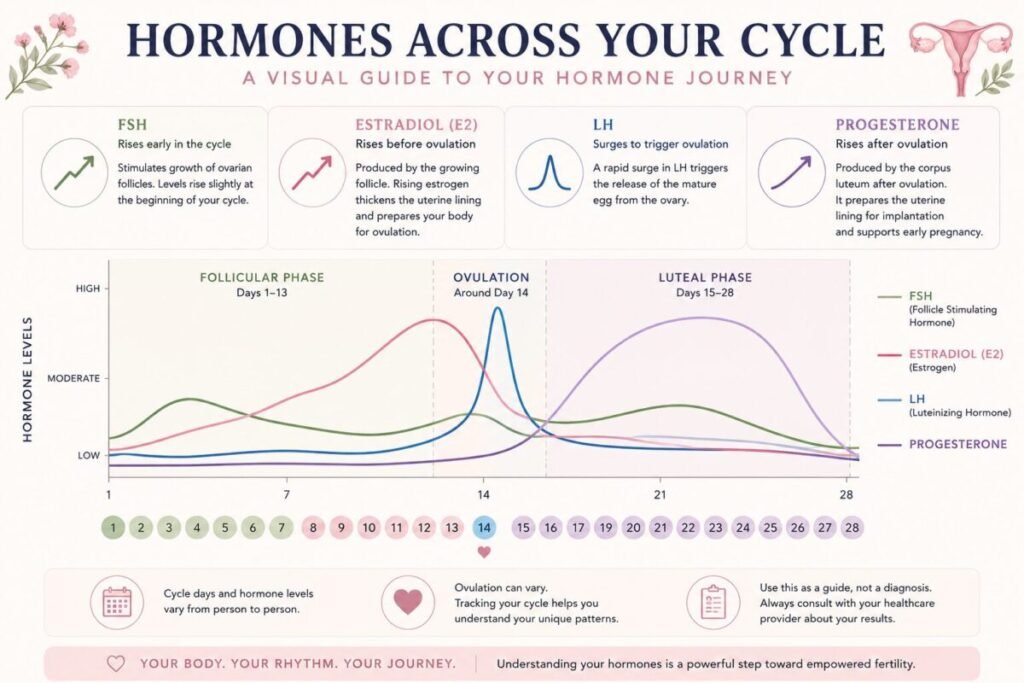
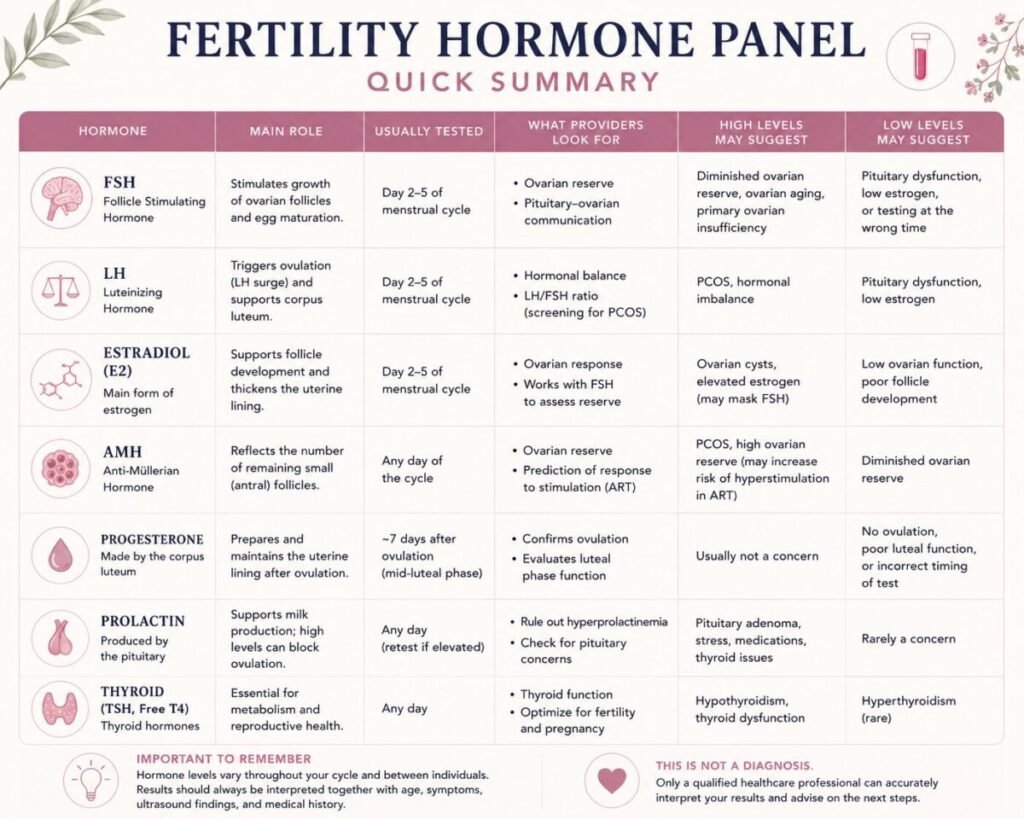
FSH: Follicle Stimulating Hormone
FSH is produced by the pituitary gland in the brain.
Its role is to stimulate ovarian follicles and support egg maturation.
One way to think of FSH is as the brain’s message to the ovaries:
“Let’s recruit and grow follicles for this cycle.”
When ovarian reserve declines, the ovaries become less responsive. The pituitary gland may compensate by producing more FSH.
For this reason, elevated FSH levels may suggest reduced ovarian reserve.
Common Reference Ranges (Day 2–5)
- Below 10 IU/L: generally considered reassuring
- 10–15 IU/L: may suggest declining reserve
- 15–20 IU/L: often associated with significantly reduced reserve
- Above 25–30 IU/L: may indicate severely diminished reserve
These values should always be interpreted together with age and other markers.
For example, an FSH of 12 IU/L may carry very different implications in a 28-year-old woman than in a 41-year-old woman.
Important Limitation
FSH can fluctuate considerably between cycles.
Many fertility specialists consider the highest repeated value more informative than a single isolated result.
Estradiol (E2)
Estradiol is the primary estrogen produced by developing follicles.
It plays an important role in:
- Endometrial growth
- Follicle development
- Communication between the ovaries and the brain
Early Cycle Estradiol
Early follicular phase estradiol is usually relatively low.
Many laboratories consider values below approximately 50 pg/mL reassuring in the early follicular phase.
Why Estradiol Matters Together With FSH
Estradiol suppresses FSH through negative feedback.
If estradiol is elevated at the beginning of the cycle, FSH may appear artificially lower than expected.
This means a seemingly normal FSH result can occasionally mask a reduced ovarian reserve.
For this reason, fertility specialists usually interpret FSH and estradiol together rather than separately.
LH: Luteinizing Hormone
LH is another hormone produced by the pituitary gland.
Its most famous role is triggering ovulation.
Just before ovulation, LH rises dramatically in what is known as the LH surge.
LH and PCOS
LH becomes particularly interesting when evaluating possible PCOS.
In some women with PCOS:
- LH remains chronically elevated
- Ovarian androgen production increases
- Ovulation becomes irregular
A LH:FSH ratio greater than approximately 2:1 or 3:1 may suggest PCOS, although current diagnosis is never based on this ratio alone.
AMH: Anti-Müllerian Hormone
AMH is produced by small developing follicles within the ovaries.
Unlike FSH, AMH remains relatively stable throughout the cycle and can usually be measured at any time.
Because AMH reflects the number of small recruitable follicles, it has become one of the most commonly used markers of ovarian reserve.
Common Interpretive Ranges
- Above 3–4 ng/mL: high reserve, sometimes associated with PCOS or increased stimulation response
- 1–3 ng/mL: often considered within the expected range
- 0.5–1 ng/mL: reduced ovarian reserve
- Below 0.5 ng/mL: very low ovarian reserve
What AMH Can Tell You
AMH estimates egg quantity.
What AMH Does NOT Tell You
AMH does not tell you:
- Whether you will conceive naturally
- Whether you are ovulating
- The quality of individual eggs
- Whether implantation will occur
- Whether you will become pregnant this month
A low AMH does not mean pregnancy is impossible.
Likewise, a high AMH does not guarantee fertility.
AMH is best viewed as one piece of information rather than a prediction of future fertility.
Progesterone: Confirming Ovulation
Progesterone is produced by the corpus luteum after ovulation.
Its role is to prepare the uterine lining for implantation and support early pregnancy.
When Should Progesterone Be Tested?
The ideal timing is approximately:
7 days after ovulation
rather than simply “Day 21.”
The traditional Day-21 progesterone test only applies to women with a classic 28-day cycle who ovulate around Day 14.
Interpreting Progesterone
Many fertility specialists consider:
- Above 10 ng/mL: evidence that ovulation likely occurred
- Above 15 ng/mL: often associated with strong corpus luteum function
Low progesterone may suggest:
- Anovulation
- Suboptimal luteal function
- Incorrect testing timing
This is why ovulation tracking often improves interpretation.
Prolactin
Prolactin is best known for supporting breast milk production.
However, elevated prolactin can interfere with ovulation by suppressing reproductive hormones.
Causes of Elevated Prolactin
- Stress
- Poor sleep
- Certain medications
- Pituitary disorders
Interestingly, anxiety surrounding the blood draw itself can temporarily elevate prolactin levels.
An unexpected result is often repeated before further investigation.
Very elevated levels may warrant additional assessment of the pituitary gland.
Thyroid Hormones: TSH and Free T4
The thyroid and reproductive system are closely connected.
Even mild thyroid dysfunction may affect:
- Menstrual regularity
- Ovulation
- Implantation
- Pregnancy outcomes
TSH and Fertility
Although laboratory reference ranges often extend to 4–5 mIU/L, many fertility specialists prefer to see TSH below approximately 2.5 mIU/L when pregnancy is desired.
This does not mean a TSH of 3.0 automatically prevents pregnancy.
Rather, some clinicians consider optimization beneficial before conception.
Summary
Common Misconceptions About Fertility Hormones
❌ Low AMH means you cannot get pregnant.
✅ Low AMH reflects ovarian reserve, not whether pregnancy is possible.
❌ High AMH means fertility is excellent.
✅ High AMH may be seen in PCOS and does not guarantee regular ovulation.
❌ A normal hormone panel means everything is fine.
✅ Fertility also depends on sperm quality, tubal patency, implantation, age, and many other factors.
❌ Day-21 progesterone should always be measured on Day 21.
✅ Ideally, progesterone is measured approximately seven days after ovulation.
Looking at the Whole Picture
A fertility hormone panel is best viewed as a collection of clues rather than a final answer.
No single hormone can diagnose fertility potential.
Doctors usually combine:
- Hormone results
- AMH
- Antral Follicle Count (AFC)
- Ultrasound findings
- Menstrual history
- Age
- Symptoms
to understand the broader picture.
A hormone result should never be interpreted in isolation.
Let’s see Examples:
These examples are simplified educational illustrations. Real-life interpretation always depends on age, symptoms, ultrasound findings, menstrual cycle history, medications, overall health, and the reference ranges used by your laboratory. Similar results may be interpreted differently in different clinical situations.
Example #1: Reassuring Ovarian Reserve
Age: 30
Results:
- FSH: 6 IU/L
- Estradiol: 35 pg/mL
- AMH: 2.8 ng/mL
- Regular 28-day cycles
What might this suggest?
These values are generally consistent with a reassuring ovarian reserve.
The ovaries appear to be responding normally to hormonal signals, and the AMH level suggests a healthy number of recruitable follicles.
However, these results alone do not guarantee fertility. Factors such as sperm quality, tubal patency, endometriosis, implantation factors, and overall health also influence the ability to conceive.
Example #2: Reduced Ovarian Reserve
Age: 38
Results:
- FSH: 18 IU/L
- Estradiol: 42 pg/mL
- AMH: 0.7 ng/mL
What might this suggest?
Both the elevated FSH and lower AMH point toward reduced ovarian reserve.
This does not mean pregnancy is impossible.
Rather, it suggests that the remaining pool of follicles may be smaller than expected and that fertility specialists may recommend not delaying evaluation or treatment options.
Age remains a particularly important factor when interpreting these results.
Example #3: High Estradiol Masking FSH
Age: 40
Results:
- FSH: 8 IU/L
- Estradiol: 95 pg/mL
- AMH: 0.5 ng/mL
What might this suggest?
At first glance, the FSH level appears reassuring.
However, elevated early-cycle estradiol may suppress FSH through negative feedback.
The low AMH provides additional context and may indicate reduced ovarian reserve despite the apparently normal FSH result.
This example illustrates why fertility specialists usually interpret FSH and estradiol together rather than separately.
Example #4: A Possible PCOS Pattern
Age: 29
Results:
- LH: 14 IU/L
- FSH: 5 IU/L
- LH:FSH ratio ≈ 3:1
- AMH: 5.8 ng/mL
- Irregular cycles
What might this suggest?
This combination may sometimes be seen in women with PCOS.
Women with PCOS often have:
- Irregular ovulation
- Higher AMH levels
- Elevated LH levels
- Increased androgen production
However, PCOS cannot be diagnosed from blood tests alone. Symptoms, ultrasound findings, and medical history are also important.
Example #5: Confirming Ovulation
Age: 33
Results:
- Progesterone: 17 ng/mL
- Blood draw performed 7 days after confirmed ovulation
What might this suggest?
A progesterone level in this range generally supports that ovulation occurred and that the corpus luteum is producing progesterone appropriately.
Timing is crucial. The same result would be interpreted differently if the blood sample had been taken too early or too late.
#6: Low Progesterone — But Timing Matters
Age: 34
Results:
- Progesterone: 4 ng/mL
- Blood draw on Day 21
- Ovulation actually occurred on Day 19
What might this suggest?
The low value may simply reflect incorrect timing.
Because ovulation occurred later than expected, progesterone was measured only two days after ovulation instead of seven.
This illustrates why the phrase “Day 21 progesterone” can be misleading for women who do not ovulate on Day 14.
Real Example #7: Elevated Prolactin
Age: 31
Results:
- Prolactin: Elevated
- Cycles becoming irregular
- No pregnancy after 12 months
What might this suggest?
Elevated prolactin can interfere with ovulation by suppressing reproductive hormones.
The result would usually be repeated because:
- Stress
- Poor sleep
- Recent exercise
- Anxiety about the blood test
can temporarily raise prolactin levels.
Persistently elevated levels may require further investigation.
Example #8: Thyroid Function and Fertility
Age: 35
Results:
- TSH: 3.8 mIU/L
- Free T4: Normal
What might this suggest?
Many laboratories would consider this result within the normal range.
However, some fertility specialists may recommend optimizing thyroid function before conception, particularly if there is a history of infertility, miscarriage, or thyroid disease.
This is one example of how “normal” and “optimal for fertility” are not always identical concepts.
Example #9: High AMH Does Not Mean Better Fertility
Age: 27
Results:
- AMH: 6.5 ng/mL
- Irregular cycles
- No confirmed ovulation
What might this suggest?
A high AMH often reflects a larger number of small follicles.
While this indicates a strong ovarian reserve, it does not guarantee regular ovulation or fertility.
In some women, particularly those with PCOS, a high AMH may coexist with ovulatory dysfunction.
This example highlights the difference between having follicles and releasing a mature egg regularly.
Example #10: Low AMH and Natural Pregnancy
Age: 39
Results:
- AMH: 0.4 ng/mL
- Regular ovulation
- Normal sperm analysis
- Open fallopian tubes
What might this suggest?
A low AMH indicates a reduced ovarian reserve, but it does not predict whether a woman can conceive in a particular month.
Many women with low AMH still achieve natural pregnancies.
AMH primarily reflects the number of remaining follicles, not the ability of an individual egg to be fertilized.
Questions to Discuss With Your Healthcare Provider About Your Hormone Panel
Understanding your hormone results can help you have more meaningful conversations with your healthcare provider. Consider bringing a copy of your results and asking some of the following questions.
About Testing Timing
-
Were my hormone levels tested at the most appropriate time in my cycle?
-
Could the timing of the blood draw have affected the results?
-
Should any of the tests be repeated during a future cycle?
-
If my cycles are irregular, how might that affect interpretation?
About Ovarian Reserve
-
What do my FSH, estradiol, and AMH levels suggest about ovarian reserve?
-
How do my results compare with what is typically expected for my age?
-
Would an Antral Follicle Count (AFC) ultrasound provide additional information?
-
Are there any limitations to interpreting my ovarian reserve based on these results alone?
About Ovulation
-
Do my hormone levels suggest that ovulation is occurring regularly?
-
Was my progesterone test performed at the ideal time?
-
Are there any signs that ovulation may be delayed or inconsistent?
-
Would cycle tracking help improve interpretation of future tests?
About PCOS and Hormonal Balance
-
Do any of my results suggest possible PCOS or another hormonal condition?
-
Should additional androgen tests be considered?
-
Would an ultrasound help provide a clearer picture?
-
How do my symptoms fit with my laboratory results?
About Thyroid Function
-
Are my thyroid results optimal for fertility and reproductive health?
-
Should any additional thyroid testing be considered?
-
Could thyroid function be contributing to my symptoms or cycle patterns?
About Prolactin
-
If my prolactin is elevated, should the test be repeated?
-
Could stress, sleep, exercise, or medications have influenced the result?
-
At what point would additional evaluation be recommended?
About the Bigger Picture
-
How should these results be interpreted alongside my age, symptoms, and menstrual cycle history?
-
Are there any findings that particularly concern you?
-
Are there any additional tests that would help complete the picture?
-
What would you recommend as the next step?
Tips:
Bring your cycle tracking records, symptom notes, basal body temperature charts, ovulation test results, or cycle calendar to your appointment. These observations can sometimes provide valuable context when interpreting hormone test results and planning next steps.
Track Your Cycle for Better Timing
One of the most helpful things you can do before fertility testing is to understand your cycle as accurately as possible.
Tracking ovulation signs, cycle length, cervical mucus, basal body temperature, and symptoms can help you and your healthcare provider better interpret hormone results. It may also help ensure that blood tests such as progesterone are performed at the most appropriate time.
To support this process, you may find my Cycle and Symptom Tracking Calendar helpful. Recording your observations over several cycles can provide valuable information and make discussions with your healthcare provider more productive.
Most importantly, remember that hormone results are only one part of your story. Whether your results bring reassurance or raise new questions, you deserve compassionate support, accurate information, and a healthcare team that helps you navigate the next steps with confidence.
The Emotional Side of Fertility Testing
Receiving fertility test results can bring relief, confusion, hope, fear, or uncertainty.
Many women find themselves searching for meaning in every number and every laboratory value. It is natural to want immediate answers when you are trying to understand your fertility or reproductive health.
Remember that test results are tools for understanding your health—not judgments about your worth, femininity, or future chances of becoming a parent.
Taking time to process information, ask questions, and seek appropriate support can be just as important as the tests themselves.
Stress, worry, and uncertainty are common experiences during fertility investigations. While stress alone does not explain fertility challenges, many women find that learning stress-management techniques, relaxation practices, and cycle awareness tools helps them feel more supported and empowered throughout the process.
At Vitality Flame, I offer several resources that may complement your fertility and cycle-awareness journey:
Free Fertility Hypnorelaxation Series
If you are feeling overwhelmed by fertility testing or trying to conceive, you may enjoy my free Fertility Hypnorelaxation Series. These guided sessions combine relaxation, breathing, visualization, and gentle mind-body techniques designed to support emotional well-being during the fertility journey.
Cycle-Syncing Hypnotherapy Series
For women who would like a deeper guided experience, the Cycle-Syncing Hypnotherapy Series is designed to accompany the different phases of the menstrual cycle. These sessions encourage greater body awareness, relaxation, and connection with your natural cycle rhythms.
The Aviva Method
The Aviva Method is a movement-based exercise system that focuses on pelvic circulation and reproductive health awareness.
During the nearly three decades that the Aviva Method has been practiced and taught in Hungary and internationally, instructors have received numerous reports from practitioners describing improvements in menstrual health, cycle awareness, and reproductive well-being. Some practitioners have also reported positive changes in hormone test results over time.
While these experiences are encouraging, they represent individual observations and should not be interpreted as medical evidence that the exercises will have the same effect in every case.
However, many women appreciate it as a natural and active way to support their overall reproductive wellness journey alongside appropriate medical care.
Final Thoughts
A fertility hormone panel can provide valuable insights into ovarian reserve, ovulation, hormonal balance, and reproductive health.
At the same time, laboratory values are only one part of a much larger story.
Two women with identical hormone levels may have very different fertility journeys.
The purpose of understanding your hormone panel is not to diagnose yourself but to feel more informed, empowered, and prepared when discussing your results with your healthcare team.
Medical Disclaimer
The information provided in this article is intended for educational and informational purposes only.
While understanding fertility hormones and laboratory results can help you feel more informed and prepared for discussions with your healthcare team, no blood test result should be interpreted in isolation.
Hormone levels can vary depending on age, menstrual cycle timing, laboratory methods, measurement units, medical history, medications, symptoms, ultrasound findings, and many other individual factors. Reference ranges may also differ between laboratories and countries.
The examples presented in this article are simplified educational illustrations and are not intended to diagnose, treat, or predict any medical condition.
Only a qualified healthcare professional who is familiar with your complete medical history can accurately interpret your test results and determine whether further evaluation or treatment is appropriate.
If you have concerns about your fertility, menstrual cycle, hormone levels, or reproductive health, please consult your physician, gynecologist, reproductive endocrinologist, or other qualified healthcare provider.
This article is not a substitute for professional medical advice, diagnosis, or treatment.